Q: Tell me about Marfan syndromeA: genetically disorders of connective tissueQ: Which gen?A: FBN1 gen, which has role in producing of fibrillin-1Q: Whats the main complications in cardiovascular system?A: mitral valve prolaps and aortic aneurysmQ: What is Bentall procedure?A: Bentall procedure is composite cardiac surgery operationQ: Which surgery operations involving?A: Replacement of the aortic valve, aortic root and ascending aorta, with re-implantation of the coronary arteriesQ: in which case Bentall surgery is used?A:This operation is used to treat combined aortic valve and ascending aorta disease, including lesions associated with Marfan syndrome.
Tuesday, December 27, 2016
Monday, December 26, 2016
Left Ventricle Hypertrophy(LVH) types
Q: Do you know how many types of LVH?
A: I thinlk, two types. Concentric and asymmetric(eccentric).
Q: also do you know the types of asymmetric?
A: Ofcourse. Septal and Apical.
Q: Great! Lets start talking abut them. Whats happening in concentric hypertrophy?
A: 1) without enlargement 2)thickened walls 3)capacity decreases
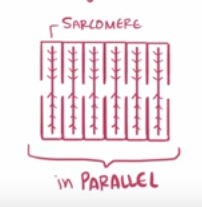
Q: How the heart walls are thickening in concentric hypertrophy?
A: New sarcomers are being added in parallel to exist one
Q: Oh, then how will be in eccentric hypertrophy?
A: In eccentric hypertrophy: New sarcomers will be added in series
A: I thinlk, two types. Concentric and asymmetric(eccentric).
Q: also do you know the types of asymmetric?
A: Ofcourse. Septal and Apical.
Q: Great! Lets start talking abut them. Whats happening in concentric hypertrophy?
A: 1) without enlargement 2)thickened walls 3)capacity decreases
Q: How the heart walls are thickening in concentric hypertrophy?
A: New sarcomers are being added in parallel to exist one

Q: Oh, then how will be in eccentric hypertrophy?
A: In eccentric hypertrophy: New sarcomers will be added in series
Tuesday, December 20, 2016
ECG case 5
What do you see?

Q: what do you see?
A: i see long RR in here.

Q: good, there is short-long-short RR. What do you see after that long RR?
A: i see a strange ritm, which looks like a VE ritm.

Q: Oh no, its not VE. If its VE, then after VE will be compensatory pause. Look attentively. You will see that is rSR' pattern and there isnt any compensatory pause. In which patology rSR' pattern finding?
A: Oh yeah! i saw rSR' pattern. I think in RBBB rSR', isnt it?
Q: Its not RBBB, its just RBBB morphology of aberrant conduction. Now, if we are talking about RBBB then what can you say about QRS duration?
A: Wide QRS?
Q: Ofcourse! These criteries are called: Ashman phenomenon. Lets repeat which criteries are finding?
A: short-long RR intervals, aberrant conducted wide QRS complex.
Q: Weldone! Dont forget, Ashman phenomen mostly observes in AF. What else you can share with us?
Wednesday, December 14, 2016
Monday, December 12, 2016
ECG case 4
what do you see?

Q: What do you see?
A: Spikes
Q: Where spikdes are locate?
A: Before each QRS complex
Q: What else do you see?
A: Large QRS complex
Q: Weldone! What else do you see?
A: LBBB pattern
Q: Oh, you are great! Then, why these patterns we see?
A: Because, this is a pacemaker rhytm.
Q: What do you see?
A: Spikes
Q: Where spikdes are locate?
A: Before each QRS complex
Q: What else do you see?
A: Large QRS complex
Q: Weldone! What else do you see?
A: LBBB pattern
Q: Oh, you are great! Then, why these patterns we see?
A: Because, this is a pacemaker rhytm.
Sunday, December 11, 2016
ECG case 3
What do you see?

Q: What do you see?
A: Shortening of the QT.
Q: Why QT is shortened?
A: Hypercalcaemia
Q: Whats the normal value of Ca in blood?
A: 8.5-10.2 mg/dL
Q: What do you see?
A: Shortening of the QT.
Q: Why QT is shortened?
A: Hypercalcaemia
Q: Whats the normal value of Ca in blood?
A: 8.5-10.2 mg/dL
ECG case 2
15 years old female patient has been found unresponsive with GCS 11/15 !
Diagnosis ?
Treatment ?


Tricyclic Overdose, Tricyclic poisoning
Diagnosis ?
Treatment ?
Tricyclic Overdose, Tricyclic poisoning
Tricyclic poisoining block sodium channel.
The two main adverse effects of sodium-channel blocker poisoning are:
1)Seizures 2)Ventricular dysrhythmias (due to blockade of sodium channels in the CNS and myocardium)
Features consistent with sodium-channel blockade are:
Interventricular conduction delay:
-QRS > 100 ms in lead II
-Right axis deviation of the terminal QRS: Terminal R wave > 3 mm in aVR
-R/S ratio > 0.7 in aVR
Patients with tricyclic overdose will also usually demonstrate sinus tachycardia secondary to muscarinic (M1) receptor blockade.
TCA toxicity with treatment: bicarbonate and hyperventilation
ECG case 1
15 years old with palpitation and dizziness b.p 120/70
Treated as Svt with vagal manoeuvre and adenosine not reverted.
Followed by IV betablocker. Get reverted to sinus rythm showing preexcitation.
is this orthdromic or antidromic?

The orthodromic adenosine if stable or shock if unstable ,
The antidromic amoidarone ,procainamide if stable and synchronized D.C. If unstable , and if in doubt treat as VT
It depend on which pathway is transmitting the impulse to the ventricle , adenosine will delay transmission in AVN in case of orthodromic , while amodarone is broad spectrum antiarrythmic will delay transmission in the accessory pathway in case of antidromic
Treated as Svt with vagal manoeuvre and adenosine not reverted.
Followed by IV betablocker. Get reverted to sinus rythm showing preexcitation.
is this orthdromic or antidromic?
The orthodromic adenosine if stable or shock if unstable ,
The antidromic amoidarone ,procainamide if stable and synchronized D.C. If unstable , and if in doubt treat as VT
It depend on which pathway is transmitting the impulse to the ventricle , adenosine will delay transmission in AVN in case of orthodromic , while amodarone is broad spectrum antiarrythmic will delay transmission in the accessory pathway in case of antidromic
Subscribe to:
Comments (Atom)
-
What do you see? Q: what do you see? A: i see long RR in here. Q: good, there is short-long-short RR. What do you see after that lon...
-
Lyme disease also known as "Lyme borreliosis" [1] Lyme disease is a systemic illness caused by the spirochete Borrelia burgdor...
-
 is used to indentify cause of SENCOPE we will identify cause of sencope: vasodepressor or cardioinhibitory patient lay on table in the s...
is used to indentify cause of SENCOPE we will identify cause of sencope: vasodepressor or cardioinhibitory patient lay on table in the s...

