Look at the image, then follow the text.
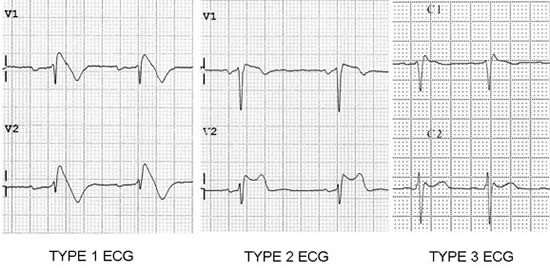
Look at the right pericordial leads (V1-V3)
Brugada type 1:
1) Coved type ST elevation
2) J point or ST elevation > 2mm
3) Negative T wave
Brugada type 2:
1) saddle-back appearance
2) J point elevation > 2mm, ST elevation > 1mm
3) Positive or Bipshasic T wave
Brugada type 3:
1) saddleback or coved appearance
2) ST-segment elevation <1 mm
Look at the right pericordial leads (V1-V3)
Brugada type 1:
1) Coved type ST elevation
2) J point or ST elevation > 2mm
3) Negative T wave
Brugada type 2:
1) saddle-back appearance
2) J point elevation > 2mm, ST elevation > 1mm
3) Positive or Bipshasic T wave
Brugada type 3:
1) saddleback or coved appearance
2) ST-segment elevation <1 mm